In remote and wilderness environments, injuries that are manageable in hospitals can quickly become life-threatening due to delayed access to medical care. Femur fractures are particularly dangerous because they cause severe pain and often substantial internal blood loss. Without rapid stabilization, patients may experience shock before reaching definitive treatment (Broken Femur). Considering that evacuation from remote areas may take hours or even days, effective field stabilization is critical.
In modern emergency medicine, traction splints are commonly used to stabilize femoral fractures during transport. These devices apply longitudinal traction to the injured leg, helping align bone fragments. By maintaining proper alignment, traction splints can reduce pain and limit additional bleeding, making them part of the pre-hospital care toolkit.
In wilderness settings, however, rescuers and outdoor travelers often lack access to specialized medical equipment. As a result, wilderness medicine training frequently teaches practitioners how to construct improvised traction splints using available materials, such as sticks or clothing.

Despite their widespread use in training, surprisingly little empirical research has evaluated the effectiveness of traction splints in prehospital care. Even fewer studies have examined whether improvised traction splints can generate adequate traction or provide stability comparable to commercially manufactured devices (Weichenthal et al., 2012). This lack of evidence raises an important question for wilderness medicine practitioners: can improvised traction splints function as reliable alternatives when commercial equipment is unavailable?
To address this question, Weichenthal and colleagues conducted a pilot study comparing an improvised traction splint with three commercially available devices. The researchers designed a prospective randomized crossover study involving 10 healthy volunteers. Each participant tested all four splints, allowing the researchers to directly compare device performance.
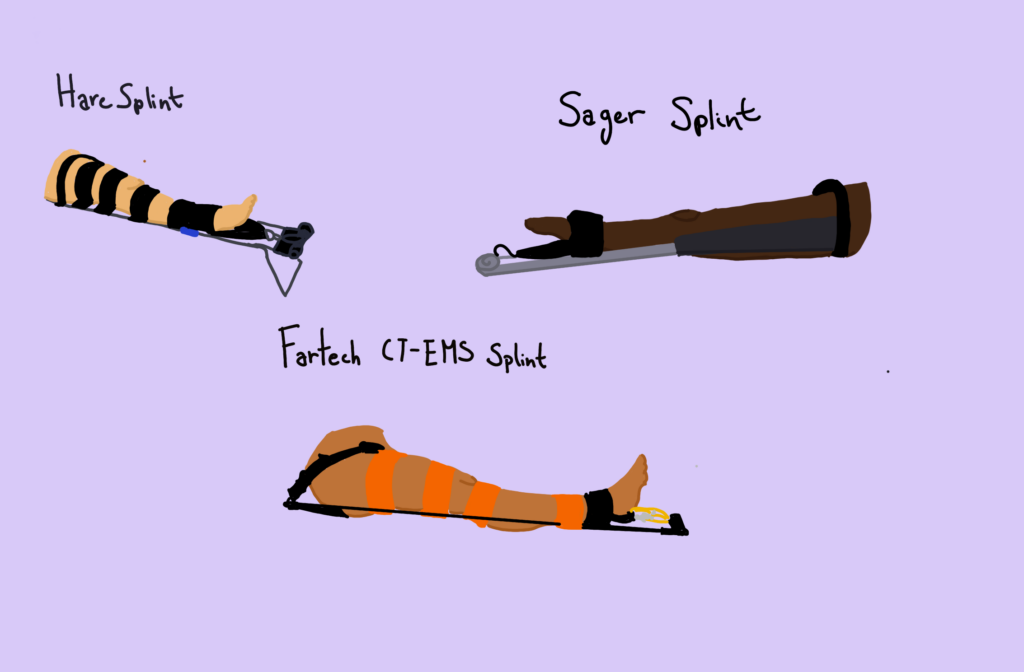
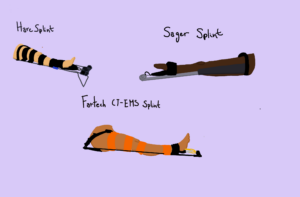
Participants were placed in four traction splints in randomized order: the Hare traction splint, the Sager splint, the Faretech CT-EMS splint, and an improvised traction splint constructed using standard wilderness first aid techniques. Each device remained in place for 30 minutes before measurements were taken.
The primary outcome measured in the study was the amount of traction force generated after 30 minutes. Traction force was measured in pounds to determine whether each splint produced clinically appropriate levels of traction. Researchers also assessed outcomes related to patient experience. After each trial, participants rated the comfort and stability of the splint on a scale from 1 to 10 and reported any side effects, such as pain or numbness.
The results showed that all four devices generated similar traction forces, ranging from 10.4 to 13.3 pounds. These values fall within the commonly recommended guideline of approximately 10 percent of a patient’s body weight, indicating that each device produced clinically adequate traction (Davis et al., 2026). Importantly, the improvised traction splint performed comparably to the three commercial splints in this primary measure.
Participants’ subjective ratings also showed minimal differences among the devices. Comfort and stability scores were similar across all four splints, suggesting that the improvised splint did not compromise the user experience. Side effects, including mild discomfort and occasional numbness, were reported with every splint tested. However, these effects were not unique to the improvised device; in fact, the improvised splint produced fewer reported side effects than some commercial splints.
Although these findings suggest that improvised traction splints may be effective, several limitations must be considered. First, the study included only 10 participants, limiting the statistical power and generalizability of the results. Larger studies would be needed to confirm these findings. Additionally, the participants were healthy volunteers rather than patients with actual femur fractures. In real injuries, pain, swelling, and muscle spasms could influence both splint performance and patient comfort. The study was also conducted in a controlled environment, not during an actual wilderness scenario. In practice, splints may remain in place for extended periods while patients are transported across uneven terrain or exposed to harsh environmental conditions. These factors could affect how effective the improvised devices are.
Despite these limitations, the study provides preliminary evidence that improvised traction splints can generate traction comparable to commercial devices while maintaining similar levels of comfort and stability. In the back country, where access to specialized equipment may be limited, the ability to improvise effective stabilization methods is an essential skill. Further research involving patients with actual femur fractures, larger participant groups, and real evacuation scenarios would help clarify the clinical effectiveness of improvised traction splints. Nevertheless, this pilot study suggests that when commercial devices are unavailable, improvised traction splints may serve as a practical and potentially effective tool for stabilizing femur fractures in wilderness settings.
This article is based on Lori Weichenthal’s Improvised Traction Splints: A Wilderness Medicine Tool or Hindrance?.
References:
Broken Femur: Causes, Symptoms, and Treatment. (n.d.). Cleveland Clinic. Retrieved May 3, 2026, from https://my.clevelandclinic.org/health/diseases/22299-broken-femur
Davis, D. D., Ginglen, J. G., Kwon, Y. H., & Kahwaji, C. I. (2026). EMS Traction Splint. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK507842/
Stick to It: Mastering the Art of Improvised Splint Techniques. (n.d.). Retrieved May 3, 2026, from https://www.sixptsurvival.com/post/stick-to-it-mastering-the-art-of-improvised-splint-techniques
Weichenthal, L., Spano, S., Horan, B., & Miss, J. (2012). Improvised Traction Splints: A Wilderness Medicine Tool or Hindrance? Wilderness & Environmental Medicine, 23(1), 61–64. https://doi.org/10.1016/j.wem.2011.12.005