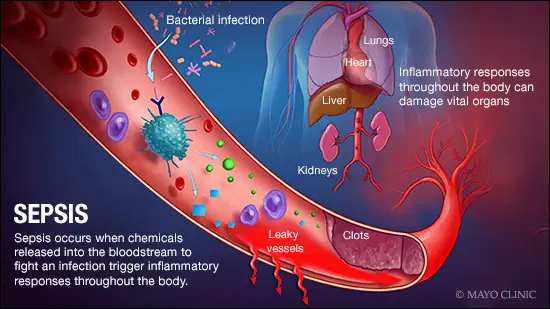
Septic shock is a severe complication of infection in which the body’s immune response becomes dysregulated. Those in septic shock experience impaired circulation, poor tissue perfusion, and ultimately organ dysfunction (What Is Septic Shock?). In pediatric patients, septic shock remains a major cause of critical illness, with mortality rates estimated between 17–32%. Pediatric cases often present differently from adult cases, most notably, children decompensate very fast and have a “cold shock” presentation. This means that rather than the vasodilation characteristic of “warm shock,” they experience low cardiac output and high vascular resistance. Essentially, children will appear stable, then quickly nosedive (Condition Topics).
To improve oxygen delivery to tissues and restore circulating blood volume, current treatment guidelines advocate rapid fluid resuscitation with 40–60 mL/kg of intravenous fluids in the first hour of sepsis and treatment. Interestingly, there is little evidence to support this guideline, and growing observational data indicate that excessive fluid administration may worsen outcomes, including increased mortality and the need for respiratory assistance. The guideline itself is based on an adult model; however, it does not translate to a pediatric situation. Alternative resuscitation techniques are becoming more popular as a result of these worries, especially if starting vasoactive drugs earlier could lessen the requirement for large fluid quantities while preserving hemodynamic stability. Hemodynamic stability refers to stable blood pressure, flow, and adequate oxygen delivery.
To investigate whether earlier initiation of vasoactive support could reduce fluid exposure in pediatric septic shock, Harley et al. conducted the Resuscitation in Pediatric Sepsis Randomized Controlled Pilot Platform Study in the Emergency Department (RESPOND ED). This was an open-label, randomized controlled study in four pediatric emergency departments throughout Australia. The trial was made up of 40 children with septic shock, ranging from 28 days to 18 years.
Children in the early-adrenaline group received an initial 20 mL/kg fluid bolus followed by early initiation of adrenaline. On the other hand, the standard-care group received 40–60 mL/kg of fluid resuscitation before administering medications that force the heart to contract (inotropes), consistent with current guidelines. A fluid bolus is the rapid administration of intravenous fluids. The primary aim of the study was to evaluate the feasibility of future related studies, while an exploratory outcome measured 28-day survival free of organ dysfunction.
This study demonstrated that the protocol was feasible. Adrenaline was given significantly earlier in the intervention group (~16 minutes) compared with the standard-care group (~49 minutes), which resulted in reduced fluid exposure. The early-adrenaline group received no additional fluid beyond the initial amount administered, while the standard-care group received around 20 mL/kg more fluid within the first 24 hours.
Clinical outcomes were similar between groups, with no mortality observed, comparable organ dysfunction–free days, and similar pediatric intensive care unit (PICU) admission rates and length of stay. Importantly, the intervention appeared safe, with no serious adverse events, such as extravasation injuries or limb ischemia associated. These circulation-based conditions are common side effects of peripheral adrenaline administration.
The RESPOND ED pilot trial demonstrates that an early-adrenaline, fluid-sparing resuscitation strategy is feasible and safe in pediatric emergency departments. While the study was not made to detect differences in mortality or major clinical outcomes, it showed that clinicians can successfully initiate vasoactive support earlier and reduce overall fluid exposure without increasing adverse events. These findings challenge the long-standing fluid-first treatment approach and suggest that earlier hemodynamic support may be a viable alternative approach. Future research will need to build on these results through larger trials, optimized dosing strategies, and broader patient populations to better determine whether early vasoactive therapy can improve outcomes and better define treatment guidelines for pediatric septic shock.
This article was based on Amanda Harley’s Early Resuscitation in Paediatric Sepsis Using Inotropes – A Randomised Controlled Pilot Study in the Emergency Department (RESPOND ED): Study Protocol and Analysis Plan.
References
Condition Topics. (n.d.). Yale Medicine. Retrieved May 3, 2026, from https://www.yalemedicine.org/conditions
Harley, A., George, S., King, M., Phillips, N., Keijzers, G., Long, D., Gibbons, K., Bellomo, R., & Schlapbach, L. J. (2021). Early Resuscitation in Paediatric Sepsis Using Inotropes – A Randomised Controlled Pilot Study in the Emergency Department (RESPOND ED): Study Protocol and Analysis Plan. Frontiers in Pediatrics, 9, 663028. https://doi.org/10.3389/fped.2021.663028
What Is Septic Shock? (n.d.). Cleveland Clinic. Retrieved May 3, 2026, from https://my.clevelandclinic.org/health/diseases/23255-septic-shock